What are Hip and Knee Replacement Implants Made Of?
AAHKS has created this guide to provide all the information and research related to materials used in hip and knee replacement surgeries. EspañolHip and knee replacement surgery involve replacing the worn-out bone and cartilage lining your hip or knee joint with new implants that are composed of materials such as ceramic, metal and plastic. The materials used for hip and knee replacements are quite similar.
Over the last two decades, the number of total hip replacements being performed each year has steadily increased in the United States. Accompanying this boom in surgery has been the release of information via the news, social media, documentaries and internet. If you’re considering hip or knee replacement surgery, it’s best to be informed by reliable sources about what is being placed inside of your body. AAHKS has created this guide to provide all the information and research related to materials used in hip and knee replacement surgeries.
Printer Friendly
See what an implant is made of:
Learn about robotic-assisted surgery:
Total Hip Replacement Materials
Standard total hip replacement implants are typically made up of approximately four individual components (see Figure 1 below):
- Stem—inserts into the femur or thigh bone
- Cup—inserts into the pelvic bone
- Ball—fits onto the end of the stem
- Liner—inserts into the cup—essentially becomes your new cartilage
The Stem
The femoral stem is the portion of the replacement that fits into your thigh bone. Historically, this is made from cobalt-chromium and/or titanium metals. In the modern era of hip replacements, cemented stems (inserted with an epoxy bone cement) are composed of cobalt-chromium metals. Cementless stems (implants in which your bone grows into the metal) are routinely made of titanium. Both designs have had excellent long-term results as part of total hip replacement systems.
- Both titanium and cobalt-chromium implants are considered highly biocompatible—meaning they are generally well tolerated by the human body with low risk of adverse reaction. In fact, both materials have been shown to be highly effective in adhering to bone.
- The top end of the femoral stem (called the trunnion) is specially shaped to hold the new ball of the artificial joint. Regardless of the material that the ball is made out of, this is where the head and stem fit together.
The Cup
The acetabulum (cup) structure fits into your pelvis and is also made from various metals. The majority of modern cups are made from titanium or tantalum metals. Both metals are well tolerated by human bone and serve as excellent surfaces for bony attachment.
- The metallic cups serve to hold the liner of the hip replacement, which essentially serves as a replacement for cartilage.
- In rare cases, the plastic liner may be used without a metallic cup and is held in place using an epoxy bone cement.
The Ball
The femoral head (ball) fits on the end of the stem (trunnion). This end of the stem is taper shaped to allow the ball to wedge into position and be held tightly in place with friction. The ball comes in varying diameters often related to the size of the cup that fits into the pelvis. The ball can be made from different materials:
- Ceramic—Many refer to this as a porcelain type material. This is a very hard surface and is extremely resistant to scratching or other damage. Ceramic heads can be paired with either ceramic or plastic liners.
- Cobalt-chromium—For the better part of the last three decades, this has been the most common material used for the ball as it is relatively-scratch resistant and holds up well (similar to ceramic described above). Cobalt-chromium heads can be paired with plastic or metal liners. Due to some potential concerns for metal debris formation when cobalt-chromium heads are paired with metal liners recently brought to light, cobalt-chromium heads are now most commonly used with plastic liners instead of metal liners.
The Liner
The acetabular liner fits into the cup and serves as your new cartilage. Much like the cartilage in your own hip, it is susceptible to wear and historically this has been the “weak link” of total hip replacement. Early forms of the liner were subject to wear by making contact with the ball and were thought to last only about 10 years. Modern day improvements have made liners last longer by either using alternative materials or strengthening the plastic.
- Ceramic—As mentioned above, ceramic is a very strong material and provides low wear rates when coupled with a ceramic ball (“ceramic-on-ceramic”).
- Cobalt-chromium—Metal liners have fallen out of favor when used with metal balls over the last 10 years; however, newer options where a plastic ball is placed in a metal liner (known as dual mobility) have shown excellent short-term results in the United States and may be useful when utilized in specific patients.
- Polyethylene—Plastic is by far the most common material used for hip replacement liners. This material has provided good to excellent results when paired with ceramic or cobalt-chromium balls. Recent advances in the manufacturing of polyethylene have significantly improved the wear rates of these plastic liners over the last 10-15 years.
When it comes time for a total hip replacement, you should discuss with your surgeon the options and pros and cons of each material. Together you can make the best decision for your particular case. While no surgical procedure is risk free or guarantees 100% success rates; remember total hip replacement is one of the most successful procedures in all of orthopedics. Many studies have shown hip implants can last beyond 15 years from the original surgery.
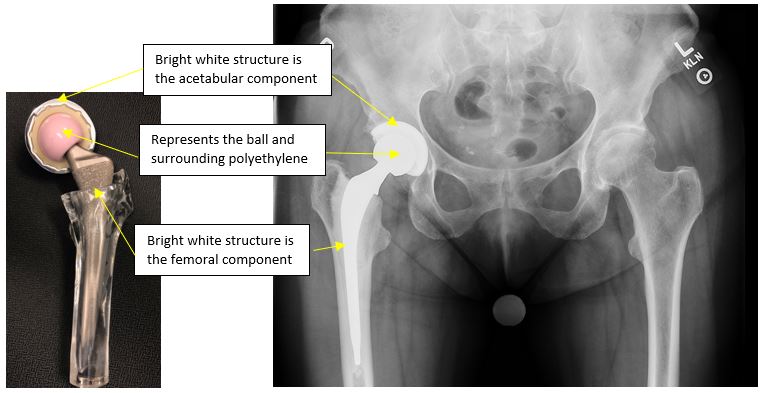
Figure 1
Total Knee Replacement Materials
Total knee replacements are made of 4 parts as well (Figure 2 – TBD):
- Femur (thigh)—top part
- Tibia—(shin) bottom piece
- Liner—serves as your new cartilage
- Patella (kneecap)—this is an optional part of the surgery, and some physicians do not use this as part of the procedure.
The Femur
Typically made from cobalt-chromium as this material is scratch resistant and safe for use in total knee replacements. The majority of total knee femoral components are made out of cobalt-chromium with excellent long-term success rates. Titanium is often too soft (scratches easily) to be a femoral component in the knee, and ceramics have a much smaller role in procedures done in the United States.
The Tibia
Made from either titanium or cobalt-chromium with excellent results for each. This portion of the replacement is meant to hold the plastic liner. Some tibial components are made of all plastic.
The Polyethylene (plastic) liner
This essentially is your new cartilage and fills the space between the two metal pieces. As with the total hip replacement, this is the “weak link” and is what will possibly wear out with time.
The Patella “button”
If your surgeon elects to use this, the undersurface of the patella (knee cap) can be covered with a piece of a plastic. This is optional, and not all surgeons routinely use this implant.
The success rate for total knee replacement is outstanding with modern implants being expected to last between 15-20 years. Similar to hip replacement, total knee replacement has been amongst the most successful orthopaedic surgeries in restoring function and quality of life. Total knee replacements have become incredibly popular in the last two decades rising at greater rates than hips (nearly a 2:1 ratio). The basic materials are the same for both hip and knee replacements, although ceramics are not routinely utilized in knee implant materials in the United States.
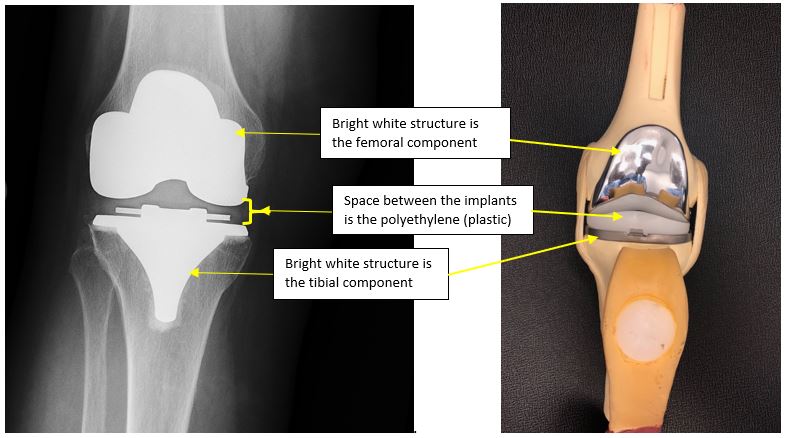
Figure 2
Long-Term Outlook
As we continue to pursue perfect hip and knee replacements, there are likely to be some designs and materials that perform better than others. The bulk materials used to make hip and knee replacements are quite similar and have not changed drastically in the last 30 years. Reaction and complications directly related to the materials themselves, while possible, are not common as manufacturer guidelines and standards are strictly followed and monitored.
The majority of total hip and knee patients can anticipate long-term success somewhere between 80-85% at 10-15 years after the surgery.
Despite recent concerns for the metals and materials used in hip and knee replacement, the vast majority of these procedures lead to successful outcomes with improvement in patients’ quality of life and function.
Talk to Your Surgeon
AAHKS recommends discussing implant options with your surgeon to gain an understanding of the particular materials to be used in your surgery.
Discuss with your surgeon the risks and benefits of different implants and materials to gain an understanding of the proposed procedure.
Developing a good relationship and level of trust with your surgeon is a key aspect of ensuring a successful outcome.
In the end, your surgeon is looking out for your best interests, and as much as you trust an airline pilot and the flight plan they follow, you should have the same trust in your surgeon.
Frequently Asked Questions
about Hip and Knee Replacement Materials
Published 2018
Once An Athlete, Always An Athlete - William Best
I've been an athlete all my life, but at age 69 was beginning to find it hard to do some of the activities I had grown fond of doing. These included skiing, horseback riding and golf. Osteoarthritis in my hip had begun to restrict my ability to twist. I decided to meet with Dr. Rafael Sierra at Mayo Rochester to discuss the possibilities of a hip replacement. During our meeting, we discussed in detail the anterior versus posterior approach to the procedure. The anterior approach seems to be the most preferred procedure these days, but with that, there's the possiblity of causing damage to the nerve bundle located near the incision. This was a concern for me. To read more, click here.
I Feel 10 Years Younger - Greg Bland
My doctor had recommended total knee replacement in 2017, but I was under the belief that I was too young (54) and that the replacement wouldn’t last very long. When the viscosupplementation finally wore off I couldn’t walk even one block before intense pain kicked in. Because of COVID-19 related delays, it took five months before I could get “elective” surgery. To read more, click here.
Expectations and Advocacy from a Well-Known Bioethics Professor - Dr. Arthur Caplan
AAHKS Patient and Public Relations Committee Chair, Dr. Brett Levine spoke with Professor and founding head of the Division of Medical Ethics at NYU Grossman School of Medicine in New York City, Dr. Arthur Caplan. Dr. Caplan had joint replacement surgery on his right knee after experiencing pain to the joint and trouble walking up stairs. From his medical school training, Dr. Caplan knew something was wrong with his knee, so he went to have it examined. Immediately upon seeing the x-ray, Dr. Caplan knew he was a candidate for knee replacement surgery. "I'm so fortunate I went early to have my knee examined, because you create more damage the longer you wait." To find out more, click here.
Years of Damage, Repaired in Hours - Rachael Epling
After being in a car accident 21 years prior, Rachael Epling decided to take her life back. As one who loves to be active, the pain she was experiencing limited her physical activities. After receiving multiple cortisone injections, trigger point injections, and radiofrequency procedures on her lower back to reduce the pain, Rachael made the toughest decision of her life. At age 42, she underwent a Total Hip Replacement via the anterior approach. It wasn't easy, but after spending half her life in pain, she was determined to get her life back. To find out more, click here.
It's all about "Work Mode" - Michelle Menconi
Michelle Menconi decided to undergo a total knee arthroplasty procedure on her right knee almost one year ago. Michelle slowly started to see her quality of life being limited due to the pain she was experiencing in her right knee. She noticed it about five years ago. To help with her deteriorating knee, she was given cortisone shots and for three weeks straight, Michelle had lubrication injected into her knee. Michelle knew it was time to do something, so she went into "work mode," handling this situation like a business transaction - doing the research to find the right surgeon for her, finding out the best way to get the surgery done, best way to recover and what she wanted long-term for her knee. To find out more, click here.
The Grateful Golfer - Rev. Dr. George B. Wirth
In March of 2017, thanks to the reference of a close friend, I flew to Little Rock to meet with, Dr. C. Lowry Barnes and his medical team to explore knee replacement for both of my knees. As a former college/graduate school rugby player for seven years in Chapel Hill, NC and Princeton, NJ, squash player and a 10K runner for 45 years, both of my knees were in bad shape. The pain had become debilitating, I had difficulty sleeping at night and walking during the day and knew that something had to be done. To read more, click here.
This article has been written and peer reviewed by the AAHKS Patient and Public Relations Committee and the AAHKS Evidence Based Medicine Committee. Links to these pages or content used from the articles must be given proper citation to the American Association of Hip and Knee Surgeons.